Cat Eye Syndrome
Cat Eye Syndrome (CES) is a rare chromosomal disorder characterized by the presence of an extra small chromosome, typically containing a partial or complete duplication of the 22q11 region. The syndrome gets its name from one of its common features: a coloboma of the iris, resembling a cat's eye. Other typical traits of CES include anal atresia with fistula, downslanting palpebral fissures, preauricular tags and/or pits, as well as congenital heart and kidney malformations. Individuals with CES generally exhibit normal or mildly impaired intellectual development, although some cases of moderate or severe intellectual disability have been reported. The incidence of CES is estimated to range from 1 in 50,000 to 1 in 150,000, with no significant difference between males and females. CES is caused by a partial tetrasomy of chromosome 22, leading to the presence of four copies of a segment of chromosome 22 instead of the usual two. This additional chromosome, often referred to as a supernumerary marker chromosome (SMC), can vary in size and shape. It may be inherited from a parent with a balanced translocation involving chromosome 22 or can occur de novo during meiosis or mitosis. The clinical manifestations of CES are highly diverse and inconsistent, ranging from asymptomatic to severe multisystem involvement. Due to this variability, diagnosing and treating CES necessitate a multidisciplinary approach that integrates various techniques and considers the unique needs and conditions of each patient.
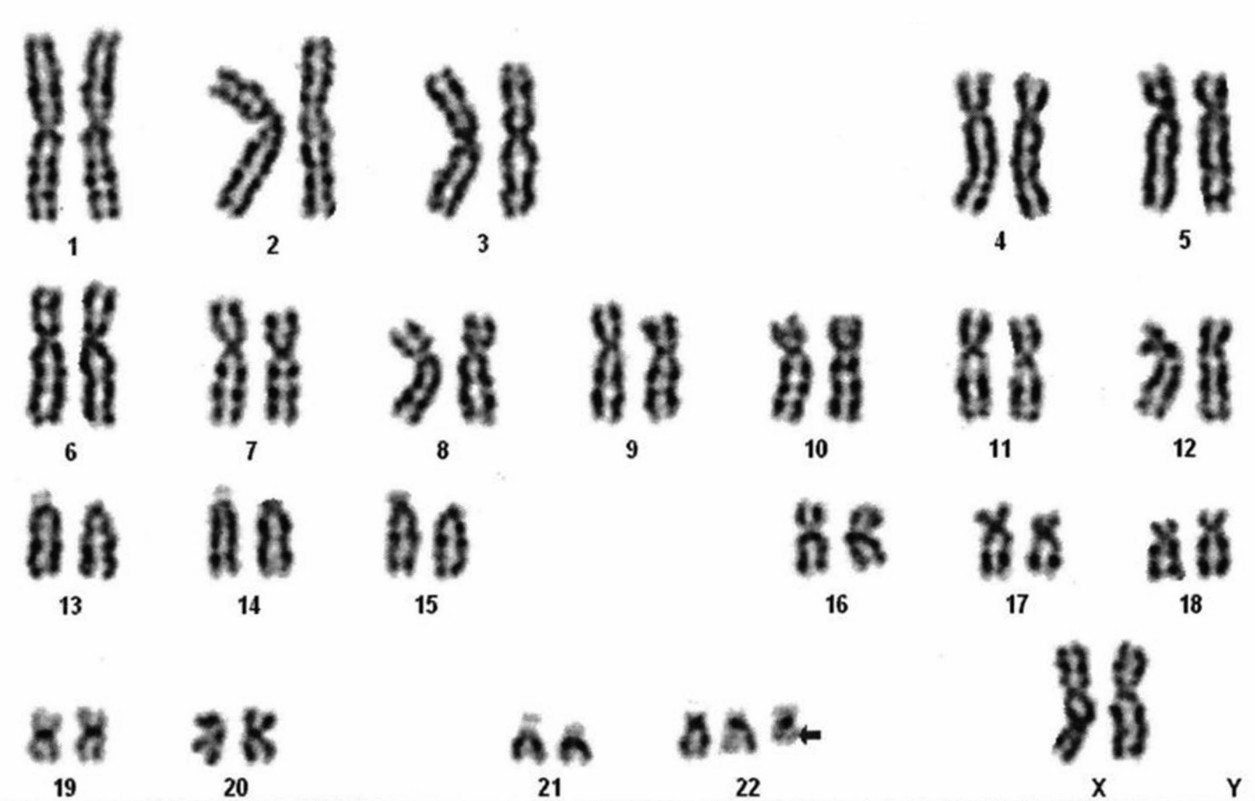 Fig.1 Karyotype of a Baby Showing 47,XX,+idic(22)(q11.2) or 47,XX,+idic(22)(pter−>q11.2::q11.2−>pter) Suggestive of CES (Sharma D, 2014)
Fig.1 Karyotype of a Baby Showing 47,XX,+idic(22)(q11.2) or 47,XX,+idic(22)(pter−>q11.2::q11.2−>pter) Suggestive of CES (Sharma D, 2014)
Clinical Features
The clinical manifestations of CES are highly variable and inconsistent, contingent upon the size and composition of the additional chromosomal fragment. This syndrome's spectrum ranges from asymptomatic cases to severe multisystem involvement. Remarkably, even within the same family, diverse phenotypes can be observed. The most prevalent features of CES include preauricular tags and/or pits—small skin growths or depressions located in front of or above the external ear canal. Although nearly all individuals with CES exhibit these traits, they are not exclusive to the syndrome and can occur in other conditions.
The second most common characteristic of CES is anal atresia, signifying the absence or obstruction of the anus, leading to difficulty or inability to pass stool. Anal atresia can be accompanied by a fistula, an abnormal connection between the rectum and organs like the bladder, vagina, or urethra in females, or the bladder, urethra, or perineum in males. This condition requires surgical correction shortly after birth.
The third prevalent feature of CES is iris coloboma, a defect in the colored part of one or both eyes that imparts the appearance of a cat's eye. Iris coloboma can impair vision and cause sensitivity to light, contingent upon the defect's size and location. Additionally, it may co-occur with other eye abnormalities like coloboma of the retina, choroid, or optic nerve, microphthalmia (small eye), aniridia (absence of iris), corneal clouding, cataracts, eyelid coloboma, and Duane syndrome (an eye movement disorder).
Clinical Diagnosis and Treatment
Diagnosing CES primarily relies on chromosomal analysis, which identifies the partial tetrasomy of chromosome 22 or other abnormalities. This analysis can employ conventional G-banding techniques or more sophisticated methods such as fluorescence in situ hybridization (FISH) or array comparative genomic hybridization (aCGH). FISH and aCGH offer higher resolution and accuracy than G-banding and can detect submicroscopic deletions or duplications potentially influencing the phenotype. CES diagnosis necessitates integrating clinical features and family history to rule out other genetic diseases or syndromes with similar symptoms. Prenatal or postnatal diagnosis can occur based on patient needs and technique availability. Ultrasound examinations during prenatal stages can hint at CES through characteristic malformations like heart defects, kidney anomalies, or skeletal abnormalities. Confirmation of prenatal diagnosis can happen through chorionic villus sampling or amniocentesis, which procure fetal cells for chromosomal analysis. Postnatal diagnosis can occur via physical examination, revealing typical features like iris coloboma, anal atresia, or preauricular tags and/or pits. Blood sampling can confirm postnatal diagnosis by providing peripheral blood lymphocytes for chromosomal analysis.
While there is no cure for CES, treatment focuses on alleviating specific features and complications. A multidisciplinary team of specialists, including geneticists, ophthalmologists, otolaryngologists, surgeons, cardiologists, nephrologists, neurologists, and others, collaborates to deliver individualized and comprehensive care. Treatment goals encompass enhancing the quality of life, reducing morbidity and mortality, and improving social and functional abilities. Available options include surgery, medication, physical therapy, and psychological therapy.
References
- Sharma D, et al. Cat eye syndrome. BMJ Case Rep. 2014 May 19;2014:bcr2014203923.
- McDermid HE, Morrow BE. Genomic disorders on 22q11. Am J Hum Genet. 2002;70(5):1077-10882.
- Gabbett MT, et al. Molecular and phenotypic aspects of chromosome 22q11.2 rearrangements. Clin Genet. 2004;66(1):14-213.
- Weber P, et al. Aniridia in a patient with cat eye syndrome: support for the involvement of chromosome region 11p13 in eye development. Am J Med Genet A. 2003;117A(2):196-198.
- Stankiewicz P, Lupski JR. Genome architecture, rearrangements and genomic disorders. Trends Genet. 2002;18(2):74-82.
- Vermeesch JR, et al. Guidelines for molecular karyotyping in constitutional genetic diagnosis. Eur J Hum Genet. 2007;15(11):1105-1114.
- Ballif BC, et al. Discovery of a previously unrecognized microdeletion syndrome of 16p11.2-p12.2. Nat Genet. 2007;39(9):1071-1073.
- Barber JC, et al. The complex relationship between phenotype and genotype in chromosome rearrangements: an international collaboration using array-CGH and FISH to investigate duplications and deletions at the distal end of chromosome 22q and the implications for genetic counselling and prenatal diagnosis in cat eye syndrome (CES). Eur J Hum Genet. 2018;26(9):1278-1290.
- Bartsch O, et al. Evidence for a new contiguous gene syndrome, the chromosome 22q11 deletion syndrome alias velo-cardio-facial syndrome alias DiGeorge syndrome alias conotruncal anomaly face syndrome alias Cayler cardiofacial syndrome alias Opitz G/BBB syndrome alias…? Am J Med Genet A. 2005;137A(3):313-315.
- McDonald-McGinn DM, et al. 22q11.2 deletion syndrome (DiGeorge syndrome/velocardiofacial syndrome). Medicine (Baltimore). 2011;90(1):1-18.