Creative Biolabs is offering the most comprehensive services for antibody development projects. With strict regulation and effective execution, we are dedicated to providing the most valuable solutions to complete your projects.
HighlightsCreative Biolabs is offering the most comprehensive services for antibody development projects. With strict regulation and effective execution, we are dedicated to providing the most valuable solutions to complete your projects.
HighlightsCreative Biolabs is offering the most comprehensive services for antibody development projects. With strict regulation and effective execution, we are dedicated to providing the most valuable solutions to complete your projects.
HighlightsCreative Biolabs is offering the most comprehensive services for antibody development projects. With strict regulation and effective execution, we are dedicated to providing the most valuable solutions to complete your projects.
HighlightsWith over a decade of experience in phage display technology, Creative Biolabs can provide a series of antibody or peptide libraries that are available for licensing or direct screening. These ready-to-use libraries are invaluable resources for isolating target-specific binders for various research, diagnostic or therapeutic applications.
HighlightsCreative Biolabs has established a broad range of platforms for developing novel antibodies or equivalents. These cutting-edge technologies enable our scientists to meet your demands from different aspects and tailor the most appropriate solution that contributes to the success of your projects.
HighlightsWith deep understanding in antibody-related realms and extensive project experience, Creative Biolabs offers a variety of references to help you learn more about our capacities and achievements, including infographic, flyer, case study, peer-reviewed publications, and all kinds of knowledge that can assist your projects. You are also welcome to contact us directly for more specific solutions.
HighlightsGet a real taste of Creative Biolabs, one of the most professional custom service providers in the world. We are committed to providing highly customized comprehensive solutions with the best quality to advance your projects.
HighlightsCurrently, autoimmune diseases of the peripheral nervous system are mainly treated with exogenous, high-dose intravenous immunoglobulin (IVIg). However, due to the increasing shortage of IVIg and other problems, it is crucial to develop new therapies, one of which is the use of B-cell-depleting monoclonal antibodies. This route has played a prominent role in the treatment of chronic autoimmune demyelinating neuropathies, particularly in anti-MAG antibody neuropathy and autoimmune neuropathies with nodal/paranoid antigen antibodies unresponsive to IVIg.
Chronic inflammatory demyelinating polyneuropathy (CIDP) is a type of inflammatory polyneuropathy characterized by progressive symmetric (lasting more than 2 months) or recurrent remitting sensorimotor deficits. Clinical studies have shown that a patient with CIDP received and responded to rituximab after the failure of IVIg and steroid therapy. In addition, the FcRn blockers efgartigimod (a humanized IgG1-derived Fc fragment that competitively inhibits FcRn) and rozanolixizumab are being investigated in CIDP.
Nodo-paranodopathies are autoimmune neuropathies. Patients with this disease respond poorly to IVIg and antibodies (mainly IgG4 and IgG3 subtypes) to nodal-paranodal antigens (i.e., neurofascial-155, contactin-1, and caspr1 in the region of the paranodal, and neurofascin-186/-140 in the region of the nodal). Clinical studies have shown that this type of disease appears to respond to rituximab. In addition, one patient responded to daratumumab, an anti-CD38 monoclonal antibody targeting long-lived plasma cells, after the failure of multiple therapies, including steroids, plasma exchange, and rituximab.
Neuropathy with anti-MAG antibodies is the most common IgM paraproteinemic neuropathy and is characterized by predominant sensory symptoms, ataxic gait, and upper limb tremors, with motor involvement and disability occurring late in the course of the disease. Clinical studies have demonstrated that the administration of rituximab improves the disability caused by anti-MAG neuropathy. However, there are very few immunotherapies that are effective in treating anti-MAG neuropathy. Thus, it is necessary to develop monoclonal antibodies that are more effective against B-cell depletion.
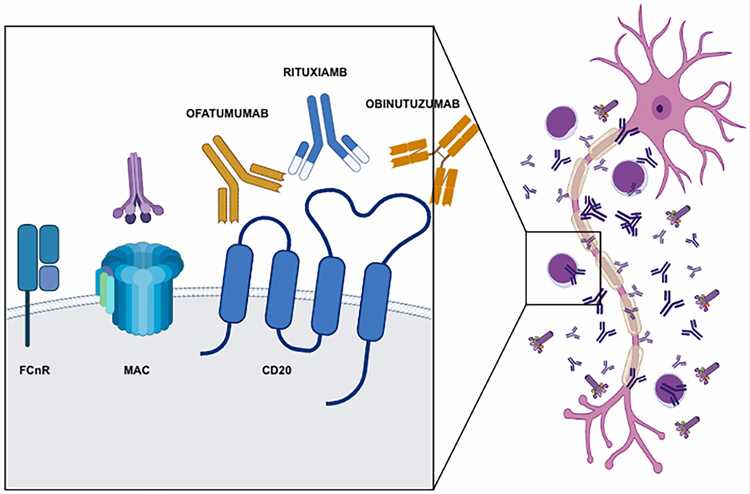 Fig 1. Neonatal Fc receptor, complement membrane attack complex (MAC), CD20, and monoclonal antibodies targeting CD20. (Chiara Briani, et al. 2022)
Fig 1. Neonatal Fc receptor, complement membrane attack complex (MAC), CD20, and monoclonal antibodies targeting CD20. (Chiara Briani, et al. 2022)
Multifocal motor neuropathy (MMN) is a rare form of acquired motor neuropathy that primarily affects young men and is characterized by progressive asymmetric weakness without sensory loss.
MMN does not respond to steroids or plasma replacement, and the response to IVIg therapy remains unclear. A study indicated that ARGX-117 (an Fc-engineered human IgG1 inhibitory anti-C2 antibody) inhibits C2-dependent complement activation triggered by the binding of IgM anti-GM1 to motor neurons.
Reference
All listed services and products are For Research Use Only. Do Not use in any diagnostic or therapeutic applications.