Schizophrenia
Schizophrenia is a severe and chronic mental disorder that profoundly affects how a person thinks, feels, and behaves. It is characterized by distortions in perception, cognition, emotion, and social functioning. According to the World Health Organization, schizophrenia affects more than 20 million people worldwide and stands as one of the leading causes of disability. The etiology and pathogenesis of schizophrenia are complex and multifactorial, involving genetic, environmental, neurodevelopmental, and neurochemical factors. Among the genetic factors, chromosomal abnormalities have been implicated in the onset of schizophrenia. These abnormalities, which involve changes in the structure or number of chromosomes, can affect the expression and function of genes. They can be inherited from parents or arise de novo during gametogenesis or early embryonic development, impacting any chromosome and varying in size and type, including deletions, duplications, inversions, translocations, and aneuploidies. Diagnosing chromosomal abnormalities is crucial for early identification, prognosis assessment, and treatment selection for schizophrenia.
Clinical Manifestations of Schizophrenia
The clinical manifestations of schizophrenia vary widely among individuals and can change over time. Symptoms typically fall into positive, negative, and cognitive domains. Positive symptoms entail abnormal experiences or behaviors added to normal mental functions, such as hallucinations, delusions, thought disorders, and agitation. Negative symptoms involve the reduction or loss of normal mental functions, including affective flattening, alogia, avolition, and anhedonia. Cognitive symptoms indicate impaired mental processes, such as attention, memory, executive function, and social cognition. Chromosomal abnormalities are found in a significant proportion of schizophrenia patients, with chromosomes 1, 2, 15, 22, and X most frequently affected. However, the relationship between chromosomal abnormalities and schizophrenia's clinical manifestations is not deterministic or specific. Cases exist where schizophrenia patients lack chromosomal abnormalities or have these abnormalities without experiencing schizophrenia symptoms. Additionally, several factors, such as genetic background, environmental exposure, epigenetic regulation, and gene-environment interaction, can modulate the impact of chromosomal abnormalities on schizophrenia phenotypes. Therefore, more research is needed to unravel the mechanisms and pathways linking chromosomal abnormalities and schizophrenia's clinical manifestations.
Diagnosis and Treatment of Schizophrenia
The diagnosis of schizophrenia is based on criteria and methods established by the Diagnostic and Statistical Manual of Mental Disorders (DSM) and the International Classification of Diseases (ICD). It necessitates the presence of at least two of the following symptoms for a significant portion of time during a one-month period: delusions, hallucinations, disorganized speech, grossly disorganized or catatonic behavior, and negative symptoms. The diagnosis also mandates a continuous disturbance for at least six months, with at least one month of active symptoms and a significant impairment in social or occupational functioning. Diagnosis primarily relies on clinical assessment and psychological testing, but laboratory tests can also help rule out other medical conditions or substance use disorders causing psychotic symptoms. Chromosomal abnormalities are diagnosed through techniques and methods capable of detecting changes in chromosome structure or number. Diagnosis can occur prenatally or postnatally, depending on the indication and availability. Common techniques include polymerase chain reaction (PCR), electrophoresis, cytogenetics, prenatal diagnosis, and high-performance liquid chromatography (HPLC). Identifying chromosomal abnormalities aids in distinguishing schizophrenia from other psychiatric disorders with similar symptoms but different genetic causes, such as bipolar disorder, schizoaffective disorder, or 22q11.2 deletion syndrome. It also guides the selection of appropriate treatment options for schizophrenia patients based on their genetic profile, such as pharmacogenetics, gene therapy, or stem cell therapy.
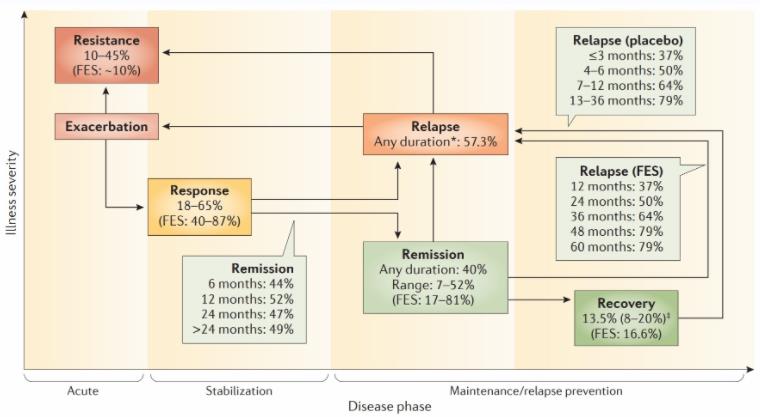 Fig.1 Treatment phases and outcomes in schizophrenia. (Kahn RS, 2015)
Fig.1 Treatment phases and outcomes in schizophrenia. (Kahn RS, 2015)
The treatment of schizophrenia aims to reduce symptoms, improve functioning, and prevent relapses. It involves both pharmacological and non-pharmacological approaches tailored to the disorder's severity, stage, and subtype. Pharmacological treatment utilizes antipsychotic drugs that modulate neurotransmitters like dopamine, serotonin, and glutamate in the brain. These drugs fall into two categories: first-generation and second-generation antipsychotics. First-generation antipsychotics, such as haloperidol, chlorpromazine, and fluphenazine, effectively treat positive symptoms but can cause extrapyramidal side effects like dystonia, akathisia, parkinsonism, and tardive dyskinesia. Second-generation antipsychotics, like clozapine, risperidone, olanzapine, and quetiapine, target negative and cognitive symptoms but may lead to metabolic side effects such as weight gain, diabetes, and dyslipidemia.
Non-pharmacological treatment involves psychological and social interventions that enhance coping skills, cognitive abilities, and social support. Psychological interventions include cognitive behavioral therapy (CBT), family therapy, psychoeducation, and cognitive remediation. Social interventions encompass vocational rehabilitation, community care, and peer support.
For the treatment of chromosomal abnormalities in schizophrenia, gene therapy principles and methods are applied. Gene therapy introduces or modifies genes in cells or tissues to correct genetic defects. This therapy can be somatic, focusing on affected cells like neurons or glia, or germline, targeting germ cells or embryos with chromosomal abnormalities such as sperm or oocytes.
References
- Avramopoulos D. Genetics of schizophrenia: an update. Mol Neuropsychiatry. 2018 Oct;4(2):59-70.
- Chen C-H, et al. Chromosomal microarray analysis as first-tier genetic test for schizophrenia. Front Genet. 2021 Oct 1;12:620496.
- Gershon ES, Alliey-Rodriguez N. New ethical issues for genetic counseling in common mental disorders. Am J Psychiatry. 2013 Sep;170(9):968-76.
- Guo T, et al. A comprehensive meta-analysis of association between genetic variants of GABAA receptor genes and schizophrenia spectrum disorders. Schizophr Res. 2018 Apr;194:35-43.
- Howie B, et al. Fast and accurate genotype imputation in genome-wide association studies through pre-phasing. Nat Genet. 2012 Aug;44(8):955-9.
- International Schizophrenia Consortium, et al. Common polygenic variation contributes to risk of schizophrenia and bipolar disorder. Nature. 2009 Aug 6;460(7256):748-52.
- Kirov G, et al. De novo CNV analysis implicates specific abnormalities of postsynaptic signalling complexes in the pathogenesis of schizophrenia. Mol Psychiatry. 2012 Feb;17(2):142-53.
- Li Z, et al. Genome-wide association analysis identifies 30 new susceptibility loci for schizophrenia. Nat Genet. 2017 Nov;49(11):1576-83.
- Marshall CR, et al. Contribution of copy number variants to schizophrenia from a genome-wide study of 41,321 subjects. Nat Genet. 2017 Jan;49(1):27-35.
- Pardiñas AF, et al. Common schizophrenia alleles are enriched in mutation-intolerant genes and in regions under strong background selection. Nat Genet. 2018 Mar;50(3):381-9.
- Ripke S, et al. Biological insights from 108 schizophrenia-associated genetic loci. Nature. 2014 Jul 24;511(7510):421-7.
- Sanders SJ, et al. Whole genome sequencing in psychiatric disorders: the WGSPD consortium. Nat Neurosci. 2017 Dec;20(12):1661-8.
- Singh T, et al. Rare loss-of-function variants in SETD1A are associated with schizophrenia and developmental disorders. Nat Neurosci. 2016 Apr ;19 (4) :571–7.
- Kahn RS, et al. Schizophrenia. Nat Rev Dis Primers. 2015 Nov 12;1:15067.
- Stefansson H, et al. Common variants conferring risk of schizophrenia. Nature. 2009 Aug ;460 (7256) :744–7.