Turner Syndrome
Turner syndrome is a genetic disorder associated with chromosomal abnormalities that primarily affects females, leading to short stature, sexual underdevelopment, infertility, and other related features. The incidence of Turner syndrome is approximately one in 2500 females, with different chromosomal types such as monosomy, mosaicism, and ring chromosomes. The diagnosis and treatment of Turner syndrome have evolved from early clinical descriptions to modern molecular diagnosis and gene therapy techniques.
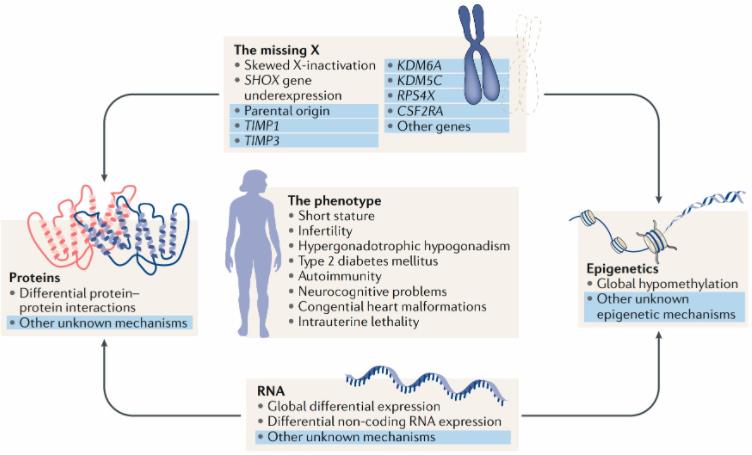 Fig.1 The phenotype and current genomic understanding of Turner syndrome. (Gravholt CH, 2019)
Fig.1 The phenotype and current genomic understanding of Turner syndrome. (Gravholt CH, 2019)
Clinical Manifestations of Turner syndrome
The clinical manifestations of Turner syndrome vary based on the chromosomal type and the patient's age. Key features include short stature, neck skin folds, flat chest, breast hypoplasia, vaginal atrophy, ovarian dysgenesis, amenorrhea, and infertility. These characteristics result from the loss of the X chromosome or its segments, containing genes crucial for growth and sexual development. Other possible features of Turner syndrome encompass cardiac malformations, renal anomalies, hearing impairment, autism, and learning difficulties. These additional traits relate to the involvement of other genes or chromosomal regions affected by abnormalities. Clinical manifestations also differ between monosomy and mosaicism types, with the former being more severe and the latter exhibiting greater variability.
Clinical Diagnosis and Treatment Methods of Turner syndrome
The methods for diagnosing and treating Turner syndrome depend on the chromosomal type and the severity of symptoms. Common clinical diagnosis techniques involve physical examination, hormone level testing, and chromosome analysis, confirming the presence of Turner syndrome and identifying the specific chromosomal type. Molecular diagnosis methods, including PCR, electrophoresis, and fluorescence in situ hybridization, accurately detect chromosomal abnormalities and establish genotype-phenotype correlations. Conventional treatment methods include growth hormone therapy, estrogen replacement therapy, and cardiac surgery, aiming to enhance growth, sexual development, and correct complications. Gene therapy methods, such as gene repair and gene transfer, attempt to restore normal gene function, preventing or curing certain symptoms.
In recent years, advancements in Turner syndrome diagnosis include the development of molecular techniques like PCR, electrophoresis, and fluorescence in situ hybridization. These methods accurately detect chromosomal abnormalities and establish genotype-phenotype correlations. Treatment options have expanded to include gene therapy methods like gene repair and gene transfer, aiming to restore normal gene function and alleviate symptoms. While these developments offer promising possibilities, challenges and limitations require further research and verification.
Conclusion
Turner syndrome, a genetic disorder associated with chromosomal abnormalities, profoundly impacts females, resulting in various physical and psychological features. Advances in diagnosis and treatment, from clinical to molecular levels, have significantly improved patients' quality of life and prognosis. Turner syndrome remains a vital and complex area of genetic disorders, shedding light on the role and function of the X chromosome and its genes. Ongoing research and future prospects, especially in molecular diagnosis and gene therapy, hold great promise for the understanding and management of Turner syndrome.
References
- Gravholt CH, et al. Turner syndrome: mechanisms and management. Nat Rev Endocrinol. 2019 Oct;15(10):601-614.
- Backeljauw PF, et al. Growth Hormone Therapy for Turner Syndrome: Evidence and Uncertainties. J Clin Endocrinol Metab. 2019 Jul 1;104(7):2495-2503.
- Bondy CA, et al. Bicuspid aortic valve and aortic coarctation are linked to deletion of the X chromosome short arm in Turner syndrome. J Med Genet. 2013 Dec;50(12):802-9.
- Bondy CA, et al. Aortic dilatation and dissection in Turner syndrome: what we know, what we are unclear about and what we should do in clinical practice? Curr Opin Endocrinol Diabetes Obes. 2014 Jun;21(3):203-10.
- Bondy CA, et al. Prenatal diagnosis of Turner syndrome: a 10-year experience. Am J Med Genet A. 2006 Jul 15;140(14):1568-73.
- Davenport ML, et al. Growth hormone treatment of early growth failure in toddlers with Turner syndrome: a randomized, controlled, multicenter trial. J Clin Endocrinol Metab. 2007 Sep;92(9):3406-16.
- Gravholt CH, et al. Clinical practice guidelines for the care of girls and women with Turner syndrome: proceedings from the 2016 Cincinnati International Turner Syndrome Meeting. Eur J Endocrinol. 2017 Sep;177(3):G1-G70.
- Hjerrild BE, et al. Turner syndrome and clinical treatment. Br Med Bull. 2010;95:139-52.
- Ho VB, et al. Major vascular anomalies in Turner syndrome: prevalence and magnetic resonance angiographic features. Circulation. 2004 Sep 14;110(11):1694-700.